Acute Invasive Fungal Sinusitis
Overview
Acute invasive fungal sinusitis (AIFS) is a life-threatening infection characterized by rapid fungal invasion of the sinonasal mucosa, submucosa, blood vessels, and adjacent structures including the orbit and central nervous system.[1] The condition predominantly affects immunocompromised patients and carries an overall mortality rate of 31.2% (95% CI, 28.3%-34.3%) according to a 2026 meta-analysis, representing significant improvement from historic mortality rates of 41.9% before 2013 to 28.2% after 2013.[2]
The disease is caused primarily by fungi of the order Mucorales (rhinocerebral mucormycosis) and Aspergillus species.[3] The pooled proportion of AIFRS among immunocompromised patients has increased to 16.6% in studies from 2013-2025, reflecting both increased incidence and improved detection.[2]
History
Arnold Paltauf coined the term "Mycosis Mucorina" in 1885 after describing the first case of systemic mucormycosis involving the sinus, brain, and gastrointestinal tract.[4][5]
In 1943, Gregory, Golden, and Haymaker at Johns Hopkins described three fatal cases of cerebral mucormycosis, establishing the clinical syndrome of rhinocerebral mucormycosis.[6] All three patients died within five days of disease onset, and for nearly a decade the condition was considered universally fatal.[5]
In 1955, Harris reported the first survivor of rhinocerebral mucormycosis, a patient who lived for 13 months following treatment.[5] Baker subsequently introduced the term "rhinocerebral mucormycosis" as a specific clinical entity.[4] The introduction of amphotericin B in the 1950s and newer antifungals (triazoles, echinocandins) has improved survival, though mortality remains substantial.[7]
Epidemiology
AIFS occurs primarily in immunocompromised patients. Risk factors include:[5][3][2]
- Hematologic malignancy: Especially acute leukemia during induction chemotherapy
- Diabetes mellitus: Particularly with diabetic ketoacidosis
- Hematopoietic stem cell transplant: Especially allogeneic HSCT with GVHD
- Solid organ transplant
- Prolonged neutropenia
- Corticosteroid therapy
- Iron overload: Including deferoxamine therapy
COVID-19 as a risk factor: The COVID-19 pandemic led to a marked increase in AIFRS incidence, particularly in patients with diabetes, renal dysfunction, and liver disease who received corticosteroids.[8][9] This association has been termed "COVID-19-associated mucormycosis" (CAM) and was particularly prominent in regions with high diabetes prevalence.
Pathophysiology
Relevant Anatomy
The paranasal sinuses are air-filled cavities within the facial skeleton that communicate with the nasal cavity through ostia.[10] The lateral nasal wall contains the middle turbinate and uncinate process, which form the boundaries of the ostiomeatal complex.
Critical adjacent structures vulnerable to fungal invasion include:[7][10]
- Orbit: The lamina papyracea (lateral ethmoid wall) is extremely thin (0.2-0.4 mm) and provides minimal barrier to orbital extension
- Anterior cranial fossa: The cribriform plate and fovea ethmoidalis form the skull base
- Cavernous sinus: Located posteriorly, receives venous drainage from the orbit and paranasal sinuses
- Pterygopalatine fossa: Contains branches of the maxillary nerve and internal maxillary artery
- Infratemporal fossa: Contains the pterygoid muscles and mandibular nerve branches
Disease Etiology
There are many different fungal species that can be invasive, but the most common are the Zygomycetes (Mucor, Rhizopus, and Rhizomucor) and Aspergillus species.[11]
Causative organisms by frequency:[5][11]
- Rhizopus species (most common Mucorales, 47% of cases)
- Mucor species (18%)
- Aspergillus fumigatus (most common Aspergillus)
- Aspergillus flavus
- Cunninghamella species
Pathophysiologic mechanisms:
Angioinvasion: Both Mucorales and Aspergillus demonstrate tropism for blood vessel walls.[12] Fungal hyphae penetrate arterial walls, causing thrombosis, tissue infarction, and necrosis. This angioinvasive property accounts for the characteristic black, necrotic tissue (eschar) seen clinically.[12]
- Neutropenia: Absolute neutrophil count <500/μL eliminates primary phagocytic defense
- Diabetic ketoacidosis: Acidosis impairs neutrophil function; elevated glucose and iron promote fungal growth
- Corticosteroids: Impair macrophage and neutrophil function
- Iron overload: Free iron is essential for fungal growth; deferoxamine therapy and transfusion-related iron overload increase risk
Histology
Histologic evaluation is necessary to determine the species of invasion, which can influence treatment decisions with respect to antifungal coverage.[11] Mucor and Rhizopus are both characterized by broad (6-25 μm), ribbon-like, pauciseptate (few or no septa) hyphae with irregular 90-degree angle branching.[11][13] Aspergillus has narrow (3-6 μm), septate hyphae with acute 45-degree angle dichotomous branching.[3]
Special stains: Grocott-Gomori methenamine silver (GMS) and periodic acid-Schiff (PAS) stains highlight fungal elements.[13] Tissue invasion—particularly angioinvasion with vessel wall penetration and thrombosis—distinguishes invasive from non-invasive fungal disease.[11]
-
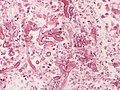
Mucormycosis
-

Mucormycosis
-

Mucormycosis with intravascular invasion
-

Aspergillosis with intravascular invasion
-

Aspergillosis with intravascular invasion, GMS stain


.jpg)
.jpg)
.jpg)
Diagnosis
Patient History
A high index of suspicion is essential in at-risk populations.[9] Key historical features include:
Immunocompromising conditions:[3][1]
- Hematologic malignancy (especially acute leukemia)
- Uncontrolled diabetes mellitus with or without ketoacidosis
- Solid organ or hematopoietic stem cell transplant
- Prolonged corticosteroid use
- HIV/AIDS
- Recent chemotherapy (within 1 month)
- Recent COVID-19 infection with corticosteroid treatment[8]
Symptom progression: Rapid onset over hours to days distinguishes AIFS from chronic invasive fungal sinusitis.[10]
- Sinonasal: Nasal congestion, purulent or bloody nasal discharge, facial pain or pressure
- Orbital: Periorbital swelling, proptosis, diplopia, vision changes
- Neurological: Altered mental status, cranial nerve deficits, severe headache
Physical Examination
Nasal endoscopy is the cornerstone of diagnosis and should be performed emergently in suspected cases:[9][11]
- Pale, ischemic, or frankly necrotic mucosa
- Black eschar on turbinates or septum (pathognomonic but late finding)
- Mucopurulent discharge
- Decreased mucosal sensation (V2 involvement)
External examination:
- Facial cellulitis, particularly V2 distribution
- Periorbital edema, proptosis, chemosis
- Ophthalmoplegia
- Palatal necrosis (indicates maxillary sinus extension)
Neurological examination:
- Cranial nerve deficits (II, III, IV, V, VI)
- Mental status changes
- Signs of Cavernous Sinus Thrombosis
Laboratory Tests
Histopathology remains the gold standard diagnostic test.[11][9]
- Tissue biopsy with frozen section: Demonstrating tissue invasion is diagnostic; frozen section analysis can also guide surgical completeness[11][14]
- Fungal cultures: From tissue specimens (not swabs); molecular techniques (DNA sequencing) aid species identification[3]
- Serum galactomannan: Specific for Aspergillus species; useful adjunct (sensitivity 70-90%)[3]
- Serum beta-D-glucan: Elevated in invasive aspergillosis but NOT useful for Mucorales[3]
- Complete blood count: Evaluate for neutropenia
- Comprehensive metabolic panel: Assess renal function, glucose, acidosis
Important: No validated serum biomarkers exist for mucormycosis; diagnosis relies on histology and/or culture with species identification.[11]
Imaging
Computed Tomography
CT is the initial imaging modality of choice.[10][3] Findings include unilateral sinus opacification, bone erosion, and extrasinus extension. CT may appear deceptively normal early in disease and typically lacks air-fluid levels (versus bacterial sinusitis).
CT Soft-Tissue Markers for Early Detection:
A 9-marker CT system has been developed where any 3 positive markers have 91.5% sensitivity and 95.9% specificity for AIFRS.[15]
A 7-variable diagnostic model (periantral fat infiltration, bone dehiscence, orbital invasion, septal ulceration, pterygopalatine fossa involvement, nasolacrimal duct involvement, lacrimal sac involvement) demonstrates that 2 or more positive variables predict AIFRS with 100% specificity.[16]
Magnetic Resonance Imaging
MRI provides superior soft tissue resolution and better delineation of orbital and intracranial extension.[16]
Key MRI findings:[17]
- "Black turbinate sign": Lack of contrast enhancement in necrotic tissue
- T2-weighted hypointensity in affected tissue
- Dural enhancement, cavernous sinus involvement
MRI prognostic findings predicting mortality:[17]
- Facial soft tissue involvement (HR 4.9)
- Nasolacrimal drainage apparatus involvement (HR 5.0)
- Intracranial involvement (HR 3.5)
MRI findings predicting visual outcomes:[17]
- Orbital apex involvement (RR 2.0 for blindness)
- Cerebral artery involvement (RR 1.8 for blindness)
Differential Diagnosis
- Acute bacterial rhinosinusitis (complicated)
- Chronic invasive fungal sinusitis
- Granulomatosis with polyangiitis (Wegener's)
- Sinonasal malignancy (squamous cell carcinoma, lymphoma)
- Necrotizing fasciitis
- Herpes zoster ophthalmicus
Management
Treatment requires the triad of surgery, antifungal therapy, and reversal of immunosuppression.[11][3]
Medical Management
Antifungal therapy should be initiated immediately upon clinical suspicion, before tissue confirmation.[11] Delayed initiation is associated with increased mortality.[18]
For Mucormycosis
First-line therapy (ECMM/MSG Guidelines):[11][19]
- Liposomal amphotericin B: 5-10 mg/kg/day IV (strongly recommended)
- Dose escalation to 10 mg/kg/day recommended for CNS involvement[19]
- Conventional amphotericin B deoxycholate is less effective and more nephrotoxic
Alternative/step-down therapy:[11][19]
- Isavuconazole: 200 mg IV/PO q8h × 6 doses (loading), then 200 mg daily — now FDA-approved for first-line treatment of mucormycosis based on comparative effectiveness data[19]
- Posaconazole: 300 mg IV/PO q12h × 2 doses (loading), then 300 mg daily
Important: Voriconazole, fluconazole, and echinocandins have NO activity against Mucorales.[11]
For Aspergillosis
First-line therapy (IDSA Guidelines):[3]
- Voriconazole: 6 mg/kg IV q12h × 2 doses (loading), then 4 mg/kg IV q12h (strongly recommended)
Alternative therapy:[3]
- Isavuconazole: As above
- Liposomal amphotericin B: 3-5 mg/kg/day (when triazoles contraindicated or unavailable)
Salvage therapy: Posaconazole, caspofungin, or combination therapy.[3]
Adjunctive Measures
- Reversal of immunosuppression when possible[11]
- Correction of diabetic ketoacidosis and hyperglycemia
- Growth factor support (G-CSF, GM-CSF) for neutropenia
- Discontinuation of deferoxamine (iron chelation)
Surgical Management
Aggressive surgical debridement is essential and strongly recommended.[11][3][1]
Principles:[14]
- Complete removal of all necrotic and infected tissue
- Debridement until bleeding, viable tissue is encountered
- Serial debridement often required (every 24-48 hours initially)
- Frozen section guidance to confirm clear margins
- Complete endoscopic resection leads to higher survival than incomplete resection[14]
Surgical approaches:[7]
- Endoscopic sinus surgery: Preferred for limited disease; allows for repeated procedures with minimal morbidity
- Open approaches: Medial maxillectomy, anterior craniofacial resection for extensive disease
- Orbital exenteration: May be required for extensive orbital invasion with loss of vision
- Palatal resection: For palatal extension
IDSA recommendation: Both surgery AND systemic antifungal therapy (voriconazole or lipid amphotericin B) should be used for invasive Aspergillus sinusitis (strong recommendation, moderate-quality evidence).[3]
Outcomes
Complications
- Orbital: Vision loss, ophthalmoplegia, Orbital Apex Syndrome
- Intracranial: Cavernous Sinus Thrombosis, meningitis, cerebritis, brain abscess, stroke
- Vascular: Internal carotid artery thrombosis, mycotic aneurysm
- Facial: Extensive tissue loss requiring reconstruction
- Systemic: Disseminated fungal infection
Prognosis
A 2026 meta-analysis found overall mortality is now 31.2% (95% CI, 28.3%-34.3%), with a notable decline from 41.9% before 2013 to 28.2% after 2013, reflecting improvements in diagnosis and treatment.[2]
Clinical Severity Staging System
A Clinical Severity Staging System was developed in 2024 to predict outcomes based on three key factors: symptom severity (local congestive vs. sensory-perceptual changes), comorbidity burden, and duration of severe neutropenia.[20]
6-month survival by stage:[20]
- Stage A: Approximately 75% survival
- Stage B: Intermediate survival
- Stage C: Approximately 15% survival
The staging system demonstrates a 57% survival gradient between best and worst stages.[20]
Prognostic Factors
Factors associated with improved survival:[20][17]
- Older age (>61 years had 29% better survival than <40 years)
- Absence of severe neutropenia (32% survival advantage)
- Lower comorbidity severity
- Orbital soft tissue involvement (paradoxically associated with decreased mortality, HR 0.3)
- Surgical treatment
- Early diagnosis and treatment initiation
- Limited sinonasal disease without extension
Poor prognostic factors:[20][17][2]
- Sensory-perceptual symptom changes (29% survival gradient)
- Prolonged severe neutropenia (>31 days)
- Intracranial extension
- Cavernous sinus involvement
- Bilateral disease
- Hematologic malignancy
- Recent bone marrow transplant
- Delayed diagnosis (>6 days from symptom onset)
MRI findings predicting mortality:[17]
- Facial soft tissue involvement (HR 4.9)
- Nasolacrimal drainage apparatus involvement (HR 5.0)
- Intracranial involvement (HR 3.5)
MRI findings predicting blindness:[17]
- Orbital apex involvement (RR 2.0)
- Cerebral artery involvement (RR 1.8)
Survivors often require long-term antifungal therapy (typically 6-12 weeks minimum) and may need reconstructive surgery for facial defects.[11]
References
- ↑ 1.0 1.1 1.2 Turner JH, Soudry E, Nayak JV, Hwang PH. Survival outcomes in acute invasive fungal sinusitis: a systematic review and quantitative synthesis of published evidence. Laryngoscope. 2013;123(5):1112-1118. doi:10.1002/lary.23912
- ↑ 2.0 2.1 2.2 2.3 2.4 Candelo E, Vasudevan SS, Osuoha GC, et al. Proportion, morbidity, and mortality of acute invasive fungal rhinosinusitis in immunocompromised populations: a systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2026. doi:10.1001/jamaoto.2025.4127
- ↑ 3.00 3.01 3.02 3.03 3.04 3.05 3.06 3.07 3.08 3.09 3.10 3.11 3.12 3.13 3.14 Patterson TF, Thompson GR 3rd, Denning DW, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;63(4):e1-e60. doi:10.1093/cid/ciw326
- ↑ 4.0 4.1 Swain SK, Sahu MC, Baisakh MR. Mucormycosis of the Head and Neck. Curr Fungal Infect Rep. 2020;14:1-11. doi:10.1007/s12281-020-00375-w
- ↑ 5.0 5.1 5.2 5.3 5.4 5.5 Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis. 2005;41(5):634-653. doi:10.1086/432579
- ↑ Gregory JE, Golden A, Haymaker W. Mucormycosis of the central nervous system. A report of three cases. Bull Johns Hopkins Hosp. 1943;73:405-419.
- ↑ 7.0 7.1 7.2 Kasapoglu F, Coskun H, Ozmen OA, et al. Acute invasive fungal rhinosinusitis: evaluation of 26 patients treated with endonasal or open surgical procedures. Otolaryngol Head Neck Surg. 2010;143(5):614-620. doi:10.1016/j.otohns.2010.08.017
- ↑ 8.0 8.1 Ismaiel WF, Abdelazim MH, Eldsoky I, et al. The impact of COVID-19 outbreak on the incidence of acute invasive fungal rhinosinusitis. Am J Otolaryngol. 2021;42(6):103080. doi:10.1016/j.amjoto.2021.103080
- ↑ 9.0 9.1 9.2 9.3 9.4 Ji J, Roland LT. Invasive fungal rhinosinusitis: current evidence and research opportunities. Curr Opin Otolaryngol Head Neck Surg. 2025;33(1):35-41. doi:10.1097/MOO.0000000000000987
- ↑ 10.0 10.1 10.2 10.3 10.4 Deutsch PG, Whittaker J, Prasad S. Invasive and non-invasive fungal rhinosinusitis—a review and update of the evidence. Medicina. 2019;55(7):319. doi:10.3390/medicina55070319
- ↑ 11.00 11.01 11.02 11.03 11.04 11.05 11.06 11.07 11.08 11.09 11.10 11.11 11.12 11.13 11.14 11.15 11.16 Cornely OA, Alastruey-Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019;19(12):e405-e421. doi:10.1016/S1473-3099(19)30312-3
- ↑ 12.0 12.1 Rapidis AD. Orbitomaxillary mucormycosis (zygomycosis) and the surgical approach to treatment: perspectives from a maxillofacial surgeon. Clin Microbiol Infect. 2009;15 Suppl 5:98-102. doi:10.1111/j.1469-0691.2009.02989.x
- ↑ 13.0 13.1 Wenig BM. Fungal Sinusitis. In: Atlas of Head and Neck Pathology. 3rd ed. Elsevier; 2016:89-95.
- ↑ 14.0 14.1 14.2 Craig JR. Updates in management of acute invasive fungal rhinosinusitis. Curr Opin Otolaryngol Head Neck Surg. 2019;27(1):29-36. doi:10.1097/MOO.0000000000000507
- ↑ John DS, Shyam K, Andrew D, Cicilet S, Deepalam SR. Utilizing CT soft-tissue markers as a screening tool for acute invasive fungal sinusitis. Br J Radiol. 2022;95(1131):20210649. doi:10.1259/bjr.20210649
- ↑ 16.0 16.1 Middlebrooks EH, Frost CJ, De Jesus RO, et al. Acute invasive fungal rhinosinusitis: a comprehensive update of CT findings and design of an effective diagnostic imaging model. AJNR Am J Neuroradiol. 2015;36(8):1529-1535. doi:10.3174/ajnr.A4298
- ↑ 17.0 17.1 17.2 17.3 17.4 17.5 17.6 Idowu OO, Soderlund KA, Laguna B, et al. Magnetic resonance imaging prognostic findings for visual and mortality outcomes in acute invasive fungal rhinosinusitis. Ophthalmology. 2022;129(10):1167-1173. doi:10.1016/j.ophtha.2022.05.011
- ↑ Chamilos G, Lewis RE, Kontoyiannis DP. Delaying amphotericin B-based frontline therapy significantly increases mortality among patients with hematologic malignancy who have zygomycosis. Clin Infect Dis. 2008;47(4):503-509. doi:10.1086/590004
- ↑ 19.0 19.1 19.2 19.3 Muthu V, Sehgal IS, Agarwal R. Treatment of pulmonary mucormycosis: current concepts. Expert Rev Anti Infect Ther. 2026;24(1):45-58. doi:10.1080/14787210.2026.2145678
- ↑ 20.0 20.1 20.2 20.3 20.4 Munyemana MA, Kallogjeri D, Chernock R, et al. Prognostic factors for survival using a clinical severity staging system among patients with acute invasive fungal sinusitis. JAMA Otolaryngol Head Neck Surg. 2024;150(2):113-120. doi:10.1001/jamaoto.2023.3811